Thiopurines: the three sisters (azathioprine, mercaptopurine and thioguanine)

Why have I been started on this medicine? Elion and Hitchings developed three related medications, the "thiopurine sisters"—thioguanine (6-TG), followed by 6-mercaptopurine (MP), and then azathioprine (AZAT) in the 1950s, later sharing the 1988 Nobel Prize in Medicine. Many inflammatory bowel disease (IBD) patients have been safely using azathioprine and mercaptopurine since the 1970s. Thioguanine has been rediscovered and is increasingly used today. These medications help control the overactive immune system in Crohn’s disease and ulcerative colitis, reducing symptoms such as intestinal bleeding, loose stools, pain, and blockages, while also allowing patients to stop steroids and avoid their long-term side effects.
How long will I need to take it to feel better? Thiopurines work slowly, typically taking 2–6 months for benefits such as reduced prednisone use, pain relief, and healing of the bowel. Some patients improve faster (20% within 2 weeks), while others take 6–12 months. If effective, AZAT/MP/6-TG is usually continued for up to 5 years or longer. In one study, 95% of patients stayed well at 1 year, 69% at 3 years, and 55% at 5 years. Stopping thiopurines increases the risk of relapse within 1–5 years and potential need for surgery, so consult your doctor before stopping.
What dose will I take? Your doctor will tell you your target dose. Dosing for azathioprine and mercaptopurine is weight-based and for tioguanine is body surface area (BSA)-based. The dose is then adjusted based on response, blood tests and thiopurine metabolite monitoring.
- Azathioprine (AZAT): 1.5–2.5 mg/kg/day - start dose 50mg daily
- Mercaptopurine (MP): 0.75–1.5 mg/kg/day - start 25mg daily
- Thioguanine (6-TG): ≤12 mg/m²/day (or 0.2–0.3 mg/kg/day) start dose 20mg daily
What options do I have if it doesn’t work? Thiopurines only work if taken consistently. "Sticking with it" or adherence can be one of the hardest parts of living with a chronic illness like Crohn’s and colitis but it is one of the most critical factors to staying well. One study showed that 70% of patients who adhered to their medication stayed well, while 50% improved even on a placebo. If AZAT/MP/6-TG has been taken correctly for 6 months and isn’t effective, or if serious side effects occur, alternative treatments may include methotrexate, biologics, research drugs, or surgery.
What are the possible side effects? Like with all drugs including placebos, a few (about 5%) get unwanted side effects, which usually improve as your body adjusts to the new medicine. Very rare potentially life-threatening reactions can occur. These effects usually go away on stopping the drug or lowering the dose. Allergy effects 2-4% in the first few weeks include fever, rash, sore joints; 3% may get abdominal pain from pancreatitis. Loss of appetite, nausea, vomiting, diarrhoea, headache, fatigue, infections, liver 0.3% or bone marrow 4% effects may occur. Severe infections (1.8%) are uncommon including chickenpox, shingles, measles and pneumonia; short viral infections are not uncommon.
How will I be monitored for the side effects? Problems usually occur in the few weeks but can occur later. Most are picked up early with blood tests (to check the bone marrow and liver). These will be carried out regularly until a stable dose has been reached (usually weekly for 4 weeks, then monthly for 3 months and then once every three months). Learn to follow these results yourself and you can usually be sent the blood results. Remember that if you are considering thiopurines, then it is likely that there are also "side effects" to doing nothing. These might include long term steroids side effects, poor quality of life from digestive symptoms, or silent damage to the gut. Again, most don't, but if you are unlucky and get unwanted side effects, it will be stopped immediately and we'll try something else.
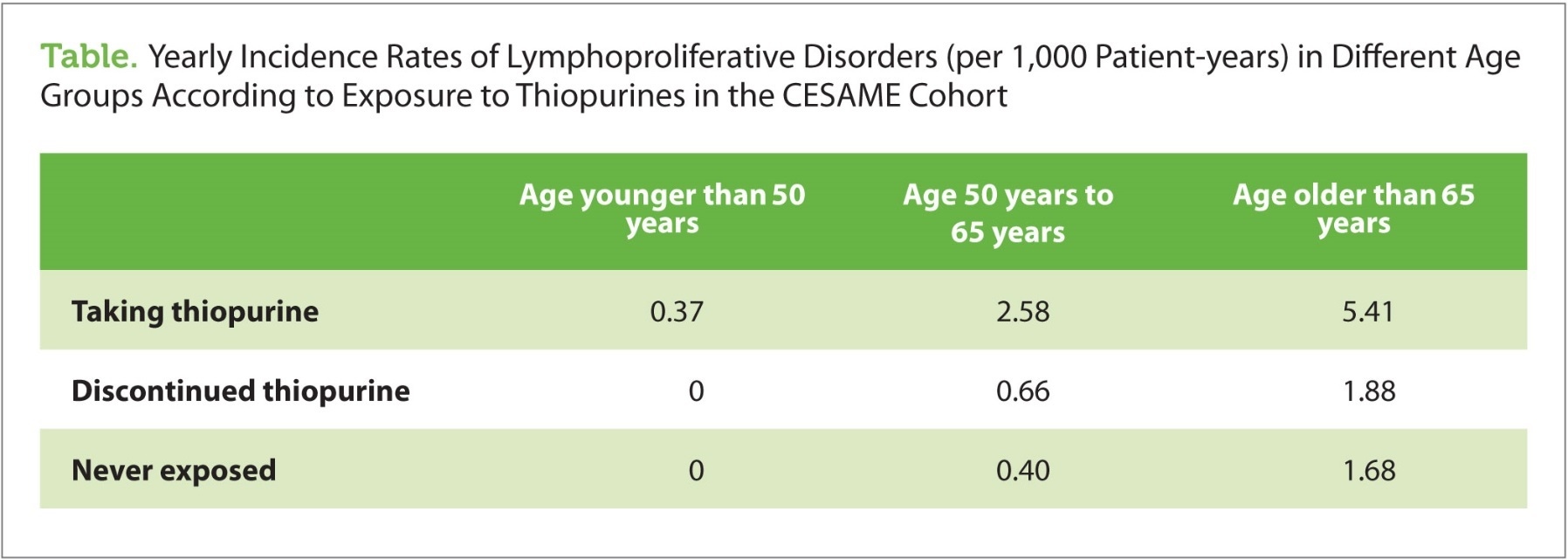
Will I need to take any special precautions while on azathioprine or 6-MP? Provided you don’t smoke, there is no strong evidence of significant increase cancer risk. Some cancers are increased and some may be prevented. Taking AZAT or MP may increase your sun sensitivity. So, be careful in the sun and avoid sunlamps, use sunscreen and get annual skin checks to help prevent skin cancer. Make sure to keep up to date with pap smears. A rare blood cancer (lymphoma) may be slightly increased in thiopurine users (2-5x increase from general very low risk of 1/2000 per year). Even though the risk remains very low, it is not clear if this is a cause or association story. Namely, it is not clear if it is the thiopurine immunomodulation that increases the risk or if it is more severe IBD activity that increases the risk and in these studies patients taking thiopurines tend to have more severe IBD activity.
Vaccines: AZAT/MP alters your immune system which can make you vulnerable to even mild infections, such as a cold or sore throat. Once on AZAT/MP never have “live vaccines” such as rubella (German measles), VZV, yellow fever and BCG; also once on AZAT/MP other vaccines don't work as well. Flu vaccines and pneumovax are safe and recommended. Check on your immunity to measles, chicken pox, hepatitis and talk with your doctor about getting these including “live vaccines” before you start AZAT/MP.
Hygiene and Infectious contacts: Wash your hands thoroughly and with antibacterial soap particularly after gardening, playing with animals and before meals. Try to avoid close contact with people who have chickenpox and tell your doctor or nurse as soon as possible if you come into contact with anyone who has any of these conditions.
Avoid taking AZAT/MP at the same time as you drink cow's milk. Cow’s milk is known to inactivate MP/AZAT. Consider carrying a medical alert identification to show you are taking AZAT/MP.
What if I get a sick on AZAT/MP? Close monitoring with your doctor helps pick up early problems. If fever, rash, sore joints or throat, bruising occurs, stop AZAT/MP until a blood test (FBC) or doctors review. Stop the drug also if blood tests are very abnormal (WBC < 3, Neutrophils < 1.5, Platelets < 150, ALT >90) and seek an urgent doctor review. See below chart. Report immediately any infections. If you have not had chicken pox, and come into contact with it or shingles, you should see your doctor quickly (within 4 days), as you may need special treatment. Don’t panic if you are the 5% who get side effects. Often with some care, under close supervision, AZAT/MP can be continued. Here you might go into remission for years after a switch from MP to AZAT or from AZAT to MP or a “desensitisation” eg. 1/8th a tablet, increasing by ¼- 1/8th of a tablet every three days until the target dose. Other reactions may respond to combining a lower dose with allopurinol.
Does AZAT/MP affect fertility, pregnancy, breastfeeding? A baby has its best start if the mother is well. Growing numbers of women safely achieve normal pregnancies, births and healthy breastfed babies on AZAT/MP. If you plan a family, or become pregnant while taking AZAT/MP, you will have to discuss the risks and benefits with your doctor and make your own balanced decision. The risk of stopping AZAT/MP may be higher than staying on it. It may help to get your IBD under control for 3 months before trying to conceive. Ensure smoking cessation, adequate B6, zinc and folate. Your doctor may recommend higher folate supplementation. AZAT/MP has not been shown to affect fertility. On breastfeeding, ask your doctor about half breast/formula feeding as it requires special care with help from an interested paediatrician or lactation consultant. In couples with miscarriage, men may consider switching to another medication, only if they have stable, inactive IBD.
Can I take other medicines at the same time? You should always tell any doctor or pharmacist treating you that you are on AZAT/MP. Some drugs don’t mix well. These include allopurinol (taken to prevent gout), warfarin (taken to stop the blood clotting), frusemide and ACE inhibitors. Be careful with over-the-counter drugs and some herbal remedies. However, most drugs can safely be taken with AZAT/MP. Ask your doctor about safe alcohol drinking.
Where can I find out more about azathioprine/mercaptopurine? If you want to know more, or if you are worried about your treatment, you should speak to your doctor or pharmacist. This information sheet does not list all of the possible side effects. For more details, look at the drug information sheet which comes in the box insert. Be reassured that, while reading about rare side effects may increase anxiety, with a little care and low risk, these drugs have helped transform the lives of many people with Crohn’s and colitis.
When should I contact my doctor? Contact your doctor or our IBD clinic in the following situations:
If you want to change your dose or stop the medicine.
If you have severe side effects.
If you are going to take any new medication or preparation.
If you are in contact with anyone who has chickenpox or shingles and you are not already immune.
If you develop any kind of infection, unusual bruising or bleeding.
If you want to start a family, become pregnant or if you want to breastfeed.
Monitoring guidelines for you and your doctor:
Bone marrow suppression (WC < 3.5 occurs up to 10%)
consider drugs interactions eg. 5-ASAs may increase neutropenia risk)
Mild (WCC 2.5-3.5): reduce AZAT/MP dose 25% and repeat FBC regularly to confirm improvement;
Moderate (WCC 1.5 - 2.5): stop AZAT/MP 1 week, & consider restarting at 50% dose with weekly FBC;
Severe (WCC < 1.5, lymphocytes <0.5 or neutrophils<1): withdraw treatment. If patient has fever admit for intravenous antibiotics and consider G-CSF.
Liver changes: consider other causes of increased ALT including drug interactions, viral illnesses, alcohol
ALT levels < 3x ULN (upper limit of normal) (ALT< 90 in 15% patients): observe as they usually resolve
ALT 3 - 10 x ULN: reduce dose by 50%, and repeat ALT in one month (if occurs at low dose specialist may consider checking metabolites eg. 6TG/6MMP, splitting dose or adding allopurinol 100mg)
ALT > 10 x greater than normal: stop drug until signs of ALT normal. Then attempt to slowly advance the dose of 6MP to the highest appropriate dose that does not cause ALT elevation.
Adult (>18yrs) Vaccine Recommendations for IBD Patients on Immunosuppression
| Vaccines recommended per routine guidelines, regardless of immunosuppression | ||||||||||||||
| Influenza (trivalent inactivated vaccine) first 2 doses 0, 4 week then annual high dose vaccine thereafter | ||||||||||||||
| Tetanus (as part of dT or dTpa) every 10 years | ||||||||||||||
HPV (quadrivalent vaccine against types 6, 11, 16, and 18)
DTap=combination vaccination against diphtheria, acellular pertussis and tetanus; HPV=human papillomavirus; MCV4=quadrivalent meningococcal vaccine; MPSV-4=quadrivalent meningococcal polysaccharide vaccine; PCV13=13-valent pneumococcal conjugate vaccine; PPSV23=23-valent pneumococcal polysaccharide vaccine Click here for further Australian guidelines |
||||||||||||||